
Calculate adjusted opioid dosages for patients with liver disease based on severity and medication type
Select liver severity and opioid type to see recommendations
Opioids can be dangerous with liver disease. Always monitor for:
When someone has liver disease, taking opioids for pain isn’t as simple as it seems. The liver doesn’t just process food and toxins-it’s the main factory that breaks down most pain medications, including morphine, oxycodone, and others. When the liver is damaged, that factory slows down or shuts off parts of its production line. The result? Opioids build up in the body, leading to dangerous side effects like extreme drowsiness, breathing problems, and even coma. This isn’t theoretical-it happens in real patients, often because doctors don’t adjust doses properly.
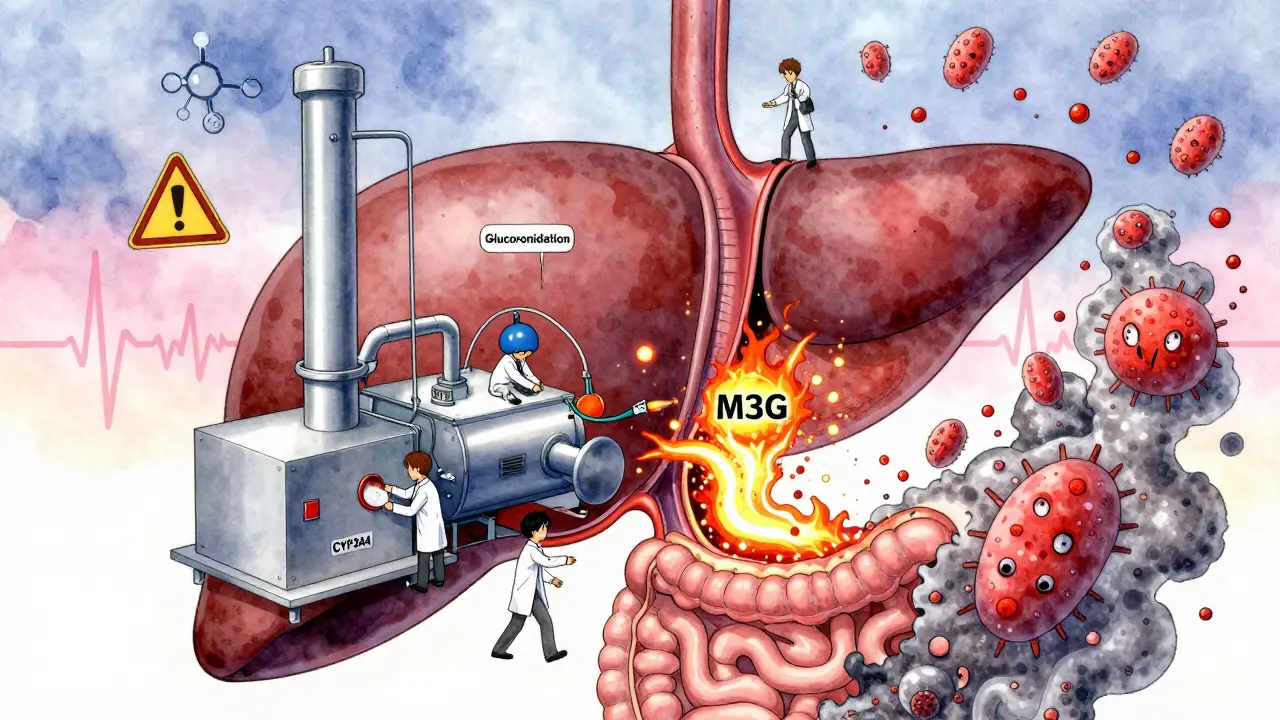
The liver uses two main systems to clear opioids from the blood: cytochrome P450 enzymes and glucuronidation. These are like specialized workers in a chemical plant. CYP3A4 and CYP2D6 are two key enzymes that handle drugs like oxycodone. Morphine, on the other hand, relies heavily on glucuronidation, turning into two different metabolites: morphine-6-glucuronide (M6G), which helps with pain relief, and morphine-3-glucuronide (M3G), which can cause seizures and confusion. In a healthy liver, these compounds are made and cleared quickly. But in liver disease, the enzymes don’t work right, and the metabolites stick around.
Studies show that in people with advanced liver failure, oxycodone’s half-life-the time it takes for half the drug to leave the body-jumps from a normal 3.5 hours to an average of 14 hours, and sometimes as long as 24 hours. That means a single dose can linger for days. Morphine’s clearance drops by up to 50% in moderate liver disease, and the risk of M3G buildup increases sharply. Even small, standard doses can become toxic.
Not all liver diseases affect opioid metabolism the same way. In alcohol-related liver disease, the enzyme CYP2E1 becomes overactive, which can speed up the breakdown of some opioids but also create more toxic byproducts. In non-alcoholic fatty liver disease (NAFLD) or diabetes-related liver damage, CYP3A4 activity drops, meaning drugs like oxycodone and fentanyl aren’t cleared efficiently. This creates a dangerous mismatch: patients with NAFLD may need lower doses than those with alcoholic cirrhosis, even if both have the same Child-Pugh score.
Another hidden risk comes from gut health. Chronic opioid use changes the balance of bacteria in the intestines. This gut microbiome imbalance triggers inflammation that travels straight to the liver through the portal vein. In someone with existing liver damage, this extra inflammation can make things worse, creating a cycle where pain meds harm the liver, and a damaged liver makes the meds more dangerous.
There’s no one-size-fits-all rule, but expert guidelines give clear starting points:
Many clinicians still give standard doses because they don’t realize how drastically liver disease changes drug handling. A 2023 study of 1,200 patients with cirrhosis found that 68% received opioid doses that were too high based on their liver function. Nearly 1 in 5 had signs of opioid toxicity within 72 hours.
Most people know opioids cause drowsiness or constipation. But in liver disease, the side effects get worse and turn dangerous:
One real case from a Melbourne hospital in 2025 involved a 62-year-old with cirrhosis who was prescribed 10 mg of oxycodone twice daily for back pain. Within three days, he became unresponsive. His blood test showed oxycodone levels 4 times higher than normal. He survived, but only after intensive care and naloxone.
Given these risks, doctors should consider alternatives before turning to opioids:
For severe pain that can’t be controlled otherwise, opioids may still be needed-but they must be treated like high-risk drugs, not routine prescriptions.
There are still big gaps in what we know. We don’t have clear dosing rules for fentanyl, tramadol, or codeine in liver disease. We don’t know how opioid-induced liver inflammation varies between viral hepatitis, autoimmune disease, or NAFLD. And we lack validated tools to predict who will develop toxicity.
Current guidelines rely on Child-Pugh or MELD scores, but these don’t fully capture metabolic function. A patient with a MELD score of 15 might still have decent CYP3A4 activity, while another with the same score might be barely metabolizing anything. Future research needs to measure enzyme activity directly, not just liver scarring.
For now, the safest approach is this: assume liver disease means reduced opioid clearance. Start low. Go slow. Monitor closely. Never assume a dose is safe just because it’s "standard."
Yes, but with major adjustments. Even mild liver disease (like early NAFLD) can reduce opioid metabolism by 20%-30%. Start with half the usual dose and wait at least 48 hours before increasing. Avoid long-acting forms. Always use the lowest effective dose and monitor for drowsiness or confusion.
Yes, often. Morphine’s metabolite M3G builds up in liver failure and can cause neurotoxicity-seizures, hallucinations, agitation-even when pain is well-controlled. Oxycodone is often preferred because its metabolites are less toxic, though it still accumulates. Fentanyl or buprenorphine patches may be safer alternatives in some cases.
Many don’t realize how dramatically liver disease changes drug handling. Standard dosing charts don’t include liver function, and guidelines are scattered. Some doctors assume all patients with cirrhosis are the same, when in fact, metabolism varies widely based on the cause of liver damage. Education gaps and lack of clear protocols are the main reasons.
The liver damage caused directly by opioids is rare, but the indirect damage from gut inflammation and immune activation can worsen existing disease. Stopping opioids and improving gut health (through diet, probiotics, or reducing constipation) can help reduce inflammation. The liver can regenerate if the stressor is removed-especially if the underlying liver disease is also managed.
Yes. Acetaminophen (up to 2g/day), gabapentin, pregabalin, and non-drug therapies like physical therapy, acupuncture, or cognitive behavioral therapy are safer first-line options. Opioids should be reserved for severe, uncontrolled pain after other options fail, and only with careful dosing and monitoring.
For patients with liver disease, opioids aren’t just painkillers-they’re potential poisons if used without understanding the liver’s role. The key isn’t avoiding them entirely, but using them with precision, respect, and constant monitoring. Every dose should be treated like a calculated risk, not a routine prescription.
Judith Manzano
9 03 26 / 05:33 AMI’ve seen this firsthand with my mom-cirrhosis from years of alcohol, then prescribed oxycodone for back pain. She went from walking to bedridden in 72 hours. No one told us the liver was the issue. They just said, ‘It’s pain meds, it’s fine.’ I wish more docs read this post. We need better training, not just more pills.
Also, if you’re a patient with liver disease: speak up. Ask for the metabolite names. Demand dose adjustments. You’re not being difficult-you’re saving your life.
rafeq khlo
10 03 26 / 02:52 AMIt is clear that the medical establishment has failed to adapt to the physiological realities of hepatic metabolism. The data is unequivocal yet ignored. Standard dosing protocols are relics of a bygone era where liver function was assumed to be uniform across all patients. This is not negligence-it is systemic malpractice. The fact that 68 percent of cirrhotic patients receive excessive opioid doses speaks volumes about the rot in clinical guidelines.
And yet no one is held accountable. No lawsuits. No audits. Just more dead bodies and silent ICU alarms.
Morgan Dodgen
11 03 26 / 00:19 AMLet me guess… next they’ll say ‘don’t take Tylenol’ because liver ‘can’t handle it’ 😂
Meanwhile Big Pharma is quietly funding studies to prove that ‘liver disease’ is just a marketing term to sell more patches and ‘specialized’ pain meds. Fentanyl patches? Sure. But why not just inject the drug directly into the bloodstream and skip the liver entirely? Oh wait-because they don’t want you to know that. The whole system is rigged.
Also-did you know morphine-3-glucuronide is actually a synthetic compound developed in the 1980s to test immune suppression? Coincidence? I think not. #OpioiGate
Philip Mattawashish
11 03 26 / 13:14 PMYou people are so naive. You think it’s about liver enzymes? It’s about control. The system doesn’t want you to be in pain because pain makes you question. Pain makes you angry. Angry people don’t obey. So they give you opioids-then let the liver fail so you’re too weak to protest. It’s not medical ignorance-it’s social engineering.
And don’t even get me started on how acetaminophen is secretly a Trojan horse. It’s not the dose that kills you-it’s the fact that they want you to think it’s safe. Wake up.
Also-your gut bacteria are being weaponized. You think probiotics help? Nah. They’re just tracking your microbiome for the NSA. You’re being monitored through your poop.
Tom Sanders
13 03 26 / 03:38 AMbro i just take one oxycodone a day for my back and i have mild fatty liver and im fine lmao
maybe its just me but idk why everyone’s acting like this is a death sentence. just don’t go crazy with it
Jazminn Jones
14 03 26 / 01:28 AMThe clinical implications of hepatic dysfunction on opioid pharmacokinetics are not merely theoretical-they are empirically validated and documented across multiple peer-reviewed cohorts. The assertion that standard dosing is acceptable in the presence of even mild cirrhosis reflects a fundamental misunderstanding of hepatic first-pass metabolism and enzyme saturation kinetics.
Moreover, the reliance on Child-Pugh scores as a surrogate for metabolic capacity is statistically indefensible. CYP3A4 activity varies independently of fibrosis stage, and thus, dosing must be guided by functional assays-not structural imaging or serum biomarkers alone.
Until hepatology and pain management departments integrate pharmacogenomic profiling into routine practice, iatrogenic toxicity will remain endemic. This is not a gap in knowledge. It is a failure of institutional will.
Stephen Rudd
14 03 26 / 09:52 AMEveryone’s acting like this is some groundbreaking revelation. Newsflash: we’ve known this since the 1990s. The fact that doctors still don’t adjust doses isn’t because they’re ignorant-it’s because they’re lazy. And the system rewards laziness. More prescriptions = more revenue. Less monitoring = less paperwork.
Also, the idea that buprenorphine patches are ‘safer’? That’s a myth. The patch still gets absorbed systemically. It just takes longer. So now you’ve got a delayed overdose instead of an immediate one. Great.
Real solution? Stop prescribing opioids for chronic pain entirely. Use acupuncture. Use yoga. Use a damn ice pack. Stop treating pain like a math problem.
Erica Santos
14 03 26 / 20:57 PMOh wow. So the liver is a ‘factory’ and opioids are ‘poisons’ and now we’re all supposed to be terrified of pain relief? How poetic.
Let me guess-the next article will be ‘Why Breathing Is Risky for People With Lungs’?
Look, if you’re giving someone 10mg of oxycodone and they’re not in pain, that’s a problem. But if they’re in agony and their liver is failing? You don’t deny them relief-you adjust the dose. Like a doctor. Not a spreadsheet.
Also, ‘morphine is the worst’? Says who? The same people who think fentanyl patches are magic? You’re not a clinician. You’re a blogger with a flowchart.
George Vou
15 03 26 / 21:35 PMimagine being so scared of pain meds that you let someone suffer because you read a reddit post
my uncle had cirrhosis and took morphine for 3 years. he lived. he was happy. he watched his grandkids grow up. now you wanna tell him he was lucky? nah. he was treated with care. not fear.
also who the hell says 'glucuronidation' out loud like its a spell? just say 'liver breaks it down' dumbass